


1Dermatology Unit, Grande Ospedale Metropolitano “Bianchi-Melacrino-Morelli” and 2Consiglio Nazionale delle Ricerche-Istituto di Fisiologia Clinica, Section of Clinical Epidemiology and Biostatistics, Reggio Calabria, and 3Farmacology Department, Magna Grecia University, Catanzaro, Italy
Apremilast is an oral selective phosphodiesterase-4 inhibitor developed recently for psoriasis treatment. The aim of this study is to assess the real-life outcomes of use of apremilast in patients with psoriasis in everyday clinical practice. A total of 159 adult patients (90 males) with plaque psoriasis were included in the study. Fifty of the patients (31%) had psoriatic arthritis. All patients started apremilast at the time of enrolment. There was a marked improvement in Psoriasis Area and Severity Index, body surface area and Dermatology Life Quality Index scores across the follow-up period (12 months). The improvements in these scores were also consistent when the patients were stratified according to increasing body mass index. Only 10.6% of the patients discontinued apremilast, because of no response. In conclusion, apremilast is an effective and safe treatment in patients with psoriasis, and its effect is not influenced by body mass index.
Key words: psoriasis; psoriatic arthritis; apremilast; obesity; retention rate.
Accepted May 26, 2021; Epub ahead of print May 27, 2021
Acta Derm Venereol 2021; 101: adv00545.
doi: 10.2340/00015555-3846
Corr: Giovanna Malara, Dermatology Unit, Grande Ospedale Metropolitano “Bianchi-Melacrino-Morelli”, Va Vallone Petrara snc, Reggio Calabria, Italy. E-mail: giovannamalara1@gmail.com
Apremilast is an oral selective phosphodiesterase-4 inhibitor developed recently for psoriasis treatment. In 159 adult patients with psoriasis (90 males; 50 patients had psoriatic arthritis), the real-life outcomes of apremilast use were assessed in everyday clinical practice. All patients started apremilast treatment at the time of enrolment and were followed up for 12 months. There was a marked improvement in the clinical index related to disease severity and psychological distress. The effectiveness of apremilast was not influenced by body mass index. Only 10.6% of the patients discontinued apremilast, indicating that it is a safe treatment.
Psoriasis is a common chronic systemic inflammatory skin disease that affects people of all ages worldwide (1). The prevalence rate of psoriasis is highly variable, depending on the geographical area (ranging from 0.09% to 11.4%) (2), and, in the Western population, is estimated as 2–4% (1). Although the aetiology of the disease is unclear, psoriasis is widely regarded as a complex disorder caused by the interaction between inherited susceptibility alleles and environmental risk factors denominated triggers (e.g. trauma, bacterial and virus infectious diseases, smoking, stress, obesity, and alcohol consumption) (3–5). The common type is plaque psoriasis, which is characterized by inflammatory plaques on the skin. These papulo-squamous lesions, often pruritic and/or painful, can arise in a classic skin sites, such as knees, elbows, scalp, and lumbar area, but also in difficult areas of the skin (nails, scalp, palms of the hands and soles of the feet) (6). The main molecular signatures of the disease are the over-production of inflammatory cytokines that lead an alteration of the immune response. In particular, myeloid dendritic cells play a key role, secreting interleukin (IL)-12 and IL-23 that activate T-helper-cells, which produce IL-17, tumour necrosis factor (TNF), interferon (IFN)γ and IL-22. This mechanism causes premature maturation of keratinocytes, infiltration of the dermis by leukocytes, and dilatation of blood vessels, leading to hyperproliferation of the epidermal layer with consequent plaque formation (7, 8). Given its multifactorial nature, the disease may present heterogeneous manifestations; several studies have reported that one-third of patients present concomitant psoriatic arthritis (PsA), an inflammatory spondyloarthropathy, and others several metabolic diseases, such as obesity, diabetes, fatty liver disease, metabolic syndrome, and cardiovascular diseases (9–12). The complexity of the possible manifestations lead the patients to experience reduced health-related quality of life (QoL), resulting in physical and mental disability (13, 14). Treatments for psoriatic disease are numerous, they can be topical and/or photo-therapies for the patients with mild disease, whereas those with moderate-to-severe disease require traditional systemic therapies (disease-modifying anti-rheumatic drugs; DMARD), such as fumaric acid esters, retinoids, methotrexate, cyclosporine, or newer biologic systemic therapies (e.g. infliximab, adalimumab, ustekinumab, secukinumab, ixekizumab) (15, 16). Because of the chronic nature of psoriatic disease, long-term treatment is often required (17). Patients’ dissatisfaction with the current treatments often lead to reduced compliance with therapy and, consequently, worsening of the disease (18). This may be due to a deterioration in health status due to tolerability issues, safety concerns (e.g. concerns over infection or malignancy with biological agents) and lack or loss of effectiveness, but also for psychological reasons, such as the administration modality (e.g. the burden imposed by subcutaneous or intravenous routes of administration) (19,20). A therapeutic alternative for patients with psoriasis and/or PsA who fail to respond to, or have contraindications to, other systemic therapies is apremilast, an oral selective phosphodiesterase-4 (PDE4) inhibitor approved by the US Food and Drug Administration (FDA) in 2014 and by the European Medicines Agency (EMA) in 2015 (21, 22). PDE4 regulates the inflammatory response by degrading cyclic adenosine 3,5-monophosphate (cAMP), an intracellular second messenger. Inhibition of PDE4 increases the level of cAMP, which results in decreased production of pro-inflammatory cytokine (IFN-γ,TNF-α, IL-12, IL-17, and IL-23) and an increase in anti-inflammatory mediator (IL-10) (23). The efficacy and good safety profiles of apremilast have been documented by different randomized trials (24–29), whereas data on real-life prospective studies in patients with psoriasis and or PsA in treatment with apremilast are scarce (8, 30–32).
Therefore, the aim of this observational, prospective, longitudinal, real-world study is to assess the long-term real-life effectiveness, safety and tolerability of apremilast among patients with psoriasis and/or PsA, paying particular attention at drug survival (time until drug discontinuation), because this is an important factor reflecting a drug’s long-term effectiveness in real life.
The protocol was approved by the ethics committee of Unit of Dermatology, Grande Ospedale Metropolitano BMM di Reggio Calabria, Italy and all participants provided written informed consent.
Patients
This real-life prospective, observational study included a total of 159 patients with a diagnosis of plaque psoriatic (90 males; 50 patients had PsA). Adult patients (> 18 years of age) were recruited from the Unit of Dermatology of Reggio Calabria Hospital, Italy. All patients with a diagnosis of psoriasis and/or PsA were included and, at the time of enrolment, they started treatment with apremilast (incident users or new users). The drug was used according to the labelled indications and posology. At the baseline visit demographic and clinical-anamnestic data of the patients were collected, such as sex, age, height, weight, body mass index (BMI), smoking status, family history of psoriasis and/or PsA, joint involvement, age of onset of the disease, previous conventional anti-psoriatic therapies (topical, systemic and/or biologic), the presence of other comorbidities and related therapies. As for effectiveness endpoints (Psoriasis Area and Severity Index (PASI), body surface area (BSA) and Dermatology Life Quality Index (DLQI)), the patients were followed up for 1 year. Information on drug discontinuation was collected over a period of 38 months. All participants were in stable clinical condition, none were pregnant or affected by cancer or diseases in the terminal phase. Data collection was performed between 16 May 2016 and 2 February 2020.
Drug administration/dose
According to the FDA and EMA indications, all enrolled patients received apremilast according to the labelled indications and posology (10 mg per os (PO)), which was titrated up to the maintenance dose of 30 mg PO twice daily.
Inclusion/exclusion criteria
Data from both male and female consecutive patients who started treatment with apremilast, aged ≥18 years and who accepted to take part into the study, with moderate-to-severe plaque psoriasis who had failed at least one systemic therapy or relapsed immediately after achieving significant improvement or had contraindications for standard systemic therapies, were considered for inclusion in this study. According to the national prescription rules established by AIFA (Italian Medicines Agency), the PASI has to be either >10 or < 10 if special if specific areas of the body are affected (face, palm-plantar, nails, genitals). Topical anti-psoriatic treatment, but not concomitant systemic therapy for PsA and/or psoriasis, was allowed.
Outcome assessment
The severity of psoriasis was assessed with the PASI, which is a measure of the average redness, thickness, and scaling of the lesions (each graded on a 0–4 scale), weighted by the area of involvement. The percentage of BSA involved was also measured in categories of 0%, 1–3%, 4–9%, 10–20%, 21– 29%, 30–50% and 51–100%. Quality of life was assessed with the DLQI. These outcomes were collected in all patients, at baseline, 3, 6 and 12 months. Outcome variables PASI 50, PASI 75, PASI 90 and PASI 100 were also considered. Relapse was defined as loss of 50% of PASI improvement from baseline in patients who achieve a clinically meaningful response.
Safety assessment
Safety assessment was performed by analysing the adverse events (AEs) reported by the patients during treatment. The primary safety endpoint was the percentage of patients experiencing grade 3–4 AEs during 24 weeks of treatment.
Statistical analysis
Descriptive statistics were calculated for each variable, using frequencies and percentage for categorical variables, mean ± standard deviation (SD) for normally distributed data or median and interquartile range (IQR) for non-normally distributed data. As a measure of uncertainty around an estimate (see Table SI) the 95% confidence interval (95% CI) was adopted. Comparisons between 2 groups were made with Student’s t-test, Mann–Whitney test or χ2 test, while comparisons among more than 2 groups were performed by analysis of variance (ANOVA) and Kruskal–Wallis test, as appropriate. To evaluate the treatment effectiveness the following outcome variables were considered: PASI, BSA, and DLQI. The values of these measures were considered as absolute score and as median and IQR value at each patient’s visit (3, 6, and 12 months). Psoriasis severity was classified based on PASI/BSA/DLQI scores as mild when all 3 scores were < 10 and as moderate–severe when at least 1 of these parameters was ≥ 10. Safety and tolerability outcomes were evaluated by collecting the adverse events (AEs) in the course of apremilast treatment. Reasons for treatment withdrawal were also recorded as primary inefficacy, secondary failure and AEs. Kaplan–Meier statistical analysis was used to estimate the free “drug discontinuation” cumulative survival; censored patients were those who were still on treatment on May 2020 (the lock date), or patients who were lost to follow-up. The statistical significance of the PASI, BSA and DLQI changes over time was investigated by linear mixed models, a method that specifically allows missing values to be taken into account, as well as by linear regression analyses weighted by patient’s identifier. The effect of BMI on the time to drug discontinuation was investigated by Cox regression analysis. In this analysis, data were expressed as hazard ratio, 95% CI and p-value. Data analysis was performed with a standard statistical package (SPSS for Windows, Version 19, Chicago, IL, USA).
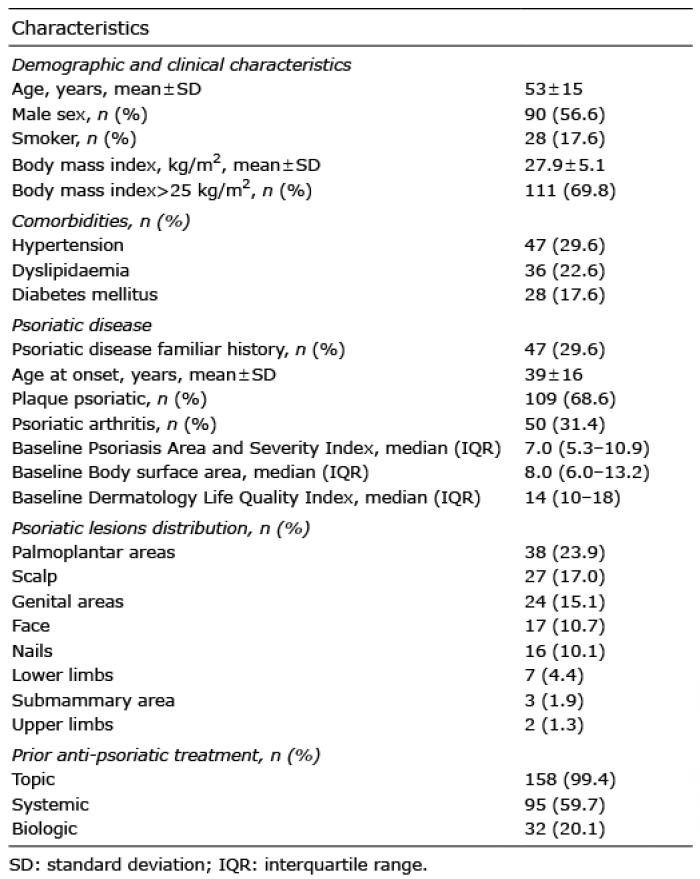
The main demographic and clinical characteristics of patients enrolled in the study are shown in Table I. Their mean age was 53 years, 57% were males and 17.6 were habitual smokers. Forty-seven patients had hypertension, 36 dyslipidaemia, and 28 were diabetic. At baseline, the median values of PASI, BSA and DLQI were 7.0, 8.0, and 14, respectively. The remaining clinical characteristics of patients are shown in Table I.
Table I. Demographic and clinical characteristics at baseline of treatment with Apremilast in a population of 159 patients with psoriasis and/or psoriatic arthritis
Longitudinal analysis of response to apremilast in the whole study sample
The evolution over time of PASI, BSA and DLQI as continuous variables as shown in Fig. 1. As plotted in the figure, both the indicators of disease severity (PASI and BSA, Fig. 1a, b) and of quality of life (DLQI, Fig. 1c) improved significantly over time. Of note, linear mixed model analysis, which accounts for missing values over time, showed that PASI, BSA and DLQI reduced by 0.58, 0.65 and 0.75 per month, and such improvements were highly significant (Fig. 1). The analysis of PASI≥50, PASI≥75, PASI≥90, and PASI 100 (Table SI) confirmed a gradual and sustained improvement in the disease across visits.
Fig. 1. Median (interquartile range) of (a) Psoriasis Area and Severity Index (PASI), (b) body surface area (BSA) and (c) Dermatology Life Quality Index (DLQI) in patients treated with apremilast at the scheduled follow-up visits (TO, T3, T6, T12).
Longitudinal analysis of response to apremilast by body mass index categories
Patients were stratified according to BMI tertiles (<25.3, 25.3–29.4 and >29.4 kg/m2). The effect of BMI on the response to apremilast in terms of PASI, BSA and DLQI was investigated by considering these outcomes as continuous variables (Fig. 2). This analysis showed a sustained improvement across visits for the disease and quality of life, which was of a similar degree across BMI categories. The same analysis by BMI strata carried out according to PASI≥50, PASI≥75, PASI≥90 and PASI 100 provided similar results (Fig. S1).
Fig. 2. Median (interquartile range) of (a) Psoriasis Area and Severity Index (PASI), (b) body surface area (BSA) and (c) Dermatology Life Quality Index (DLQI) in patients treated with apremilast at the scheduled follow-up visits (TO: white bar, T3: light-grey bar, T6: grey bar, T12: dark-grey bar) stratified according to body mass index (BMI) tertiles.
Safety and drug discontinuation
At the end of the follow-up, the majority of patients were still on treatment with apremilast (Fig. 3a), whereas 2 patients interrupted the study because of disease resolution. A total of 28 patients were lost to follow-up, 1 patient died and 17 patients discontinued the study because of no response (Fig. 3a). The Kaplan–Meier analysis of time to drug discontinuation in 17 patients who discontinued apremilast is shown in Fig. 3b. The median time to drug discontinuation was 6.3 months (95% CI 5.7–7.0 months). Of note, BMI was largely unrelated to the time to the drug discontinuation (hazard ratio 1.03, 95% CI 0.93–1.14, p = 0.56). No major adverse events were observed across the follow-up period.
Fig. 3. (a) Events during follow-up. Only 17 patients were non-responders to the apremilast treatment (10.6%); (b) Kaplan–Meier survival curve showing the time to “drug discontinuation” in 17 patients who were non-responders to apremilast. The follow-up time corresponding to the condition of 111 patients still on treatment (mean ± standard error) 11.9 ± 0.9 months. Patients “lost to follow-up” included those who changed residence and/or were unwilling to participate in the scheduled follow-up visits.
This real-life study confirms the effectiveness and safety of treatment with apremilast in patients with psoriasis, and documented that such protective effect is consistent across BMI categories.
Inflammation is an evolutionary conservative process that protects the host from bacteria, viruses, toxins and infections through the activation of immune and non-immune cells by eliminating pathogens and promoting tissue recovery and repair (33, 34). It is also the driving factor in many diseases, including infections, cancer, immune-mediated, metabolic and neurodegenerative disorders (35). For many years, non-steroidal anti-inflammatory drugs (NSAIDs) (36) and corticosteroids have made a major contribution to treating inflammatory diseases; nevertheless, their long term use can cause severe organ toxicity and several other side-effects. To date, numerous new therapeutic options, particularly designed for long-term use, have emerged for better controlling the inflammatory processes, underling the above-mentioned diseases (37–40). Beyond biologicals, which control immunological dysregulation by inhibiting extracellular inflammatory molecules (extracellular pathways), other molecules, such as apremilast, a phosphodiesterase-4 inhibitor (PDE-4), act in an intracellular manner (41). PDE4 inhibition results in the accumulation of the intracellular second messenger cAMP, downstream activation of protein kinase A (PKA), and subsequent phosphorylation of the transcription factor cAMP-response element binding protein (CREB). Activation of this pathway modulates gene transcription of numerous cytokines, and results in the suppression of TNFα production and other pro-inflammatory cytokines. PDE4 inhibition can also increase the production of anti-inflammatory cytokines from macrophages, and interfere with the phenotype and function of B cells. In addition, it can promote the barrier function of keratinocytes and epithelial cells via suppression of the inflammatory mediator production (41, 42). As a consequence of its wide anti-inflammatory activities, apremilast, a PDE4 inhibitor, has been evaluated for the treatment of several skin disorders or rheumatic diseases, such as psoriasis and PsA (41). Much of the data supporting the efficacy and safety of apremilast in the treatment of psoriasis and PsA come from clinical trials (24–29). Real-life treatment outcomes may differ from clinical trial results, due to preselected patient cohorts in clinical trials. This study documented a marked improvement in PASI, BSA and DLQI across an extended follow-up period (12 months). Indeed, PASI 75 increased from 17.7% (T0) to 69.1% (T12) and PASI 90 and PASI 100 increased from 4.2% and 2.1% (T0) to 41.2% and 20.6%, respectively, at T12. Of note, these results were confirmed by an additional analysis by linear mixed models, an analytical approach, which specifically takes into account the presence of missing values over time. The proportion of patients who achieved PASI 75 after approximately 16 weeks of treatment with apremilast was higher in a study by Papp (25) than was found in the current study (33.1% vs 17.7%). This difference probably depends on differences in baseline characteristics of patients between the 2 studies. Compared with those enrolled in the current study, patients enrolled in Papp’s study (25) were younger (46 vs 53 years) and displayed more severe disease (PASI score, 19 vs 9; BSA score, 25 vs 10). It is a consolidated notion that the higher the severity of the disease, the higher the margin of improvement. Thus, the difference in PASI 75 response rate at 3 months between the current study and Papp’s study probably depends on the higher severity of the disease in patients in Papp’s study (25). In Papp’s study, no obese patient achieved PASI 50, which may depend on the fact that only 6 patients in their study were obese. In the current study 47 patients had a BMI >30 kg/m2. The higher the number of obese patients, the greater the possibility of observing any disease improvement occurring in this patient category.
As mentioned above, psoriasis is a chronic skin inflammatory disease, with an estimated prevalence of approximately 2–3% among the Caucasian population (43), of whom 2–3% develop PsA (44). Psoriasis has also been identified as a multisystem chronic inflammatory disorder associated with multiple comorbidities, including cardio-metabolic disorders (type 2 diabetes, dyslipidaemia, metabolic syndrome, obesity, hypertension, non alcoholic liver fatty disease) and chronic kidney disease (45, 46). Patients with psoriasis are more frequently overweight or obese than the general population, and the severity of psoriasis correlates with BMI (47).
The current study found that the improvements in PASI (either as continuous (Fig. 2) or categorical (Fig. S1) variables), BSA and DLQI were consistent across BMI categories indicating that overweight/obesity does not affect the real-life effectiveness of apremilast in patients with psoriasis. The pathophysiological mechanisms connecting psoriasis and obesity lie in the increased systemic inflammation induced by adipose tissue, particularly by visceral adipose tissue, which acts as an endocrine organ releasing adipokines. The between pro- and anti-inflammatory adipokines imbalance in obsesity provides the development of a chronic low-grade inflammatory state, which could trigger or worsen psoriasis (48). In psoriatic patients, obesity may predict lower efficacy for systemic conventional and biologic drugs, especially for those with fixed-dose (49, 50). However, no meaningful effect of BMI on the effectiveness of apremilast was found in the current study.
In the study population, only 17 patients out of 159 (i.e. 10.6%) discontinued apremilast because of no response, and the Kaplan–Meier analysis in these patients showed that the median time to drug discontinuation was 7 months. No grade 3/4 AEs were observed across the follow-up period. The difference in the number of AEs between the current study and that of Vujic et al. (8) can be explained by the fact that the current study protocol involved collection only of grades 3–4 AEs.
In conclusion, apremilast is an effective and safe treatment in patients with psoriasis, and this effect is not influenced by BMI.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize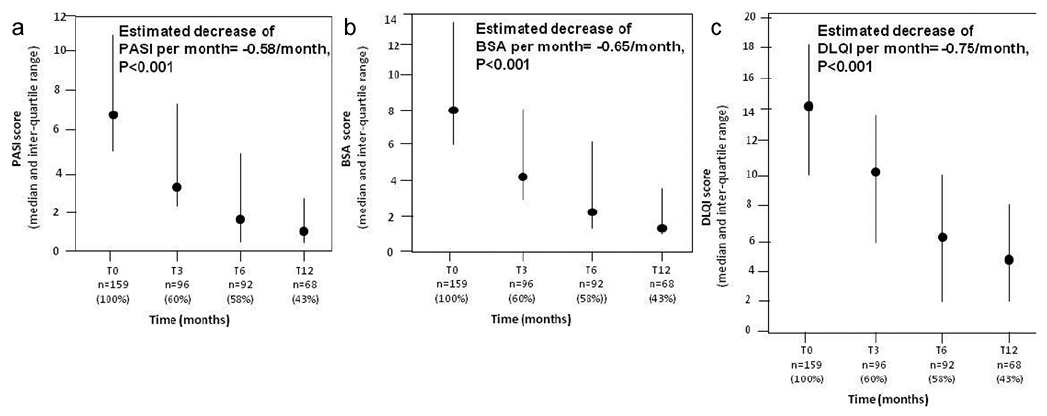 Click to show fullsize
Click to show fullsize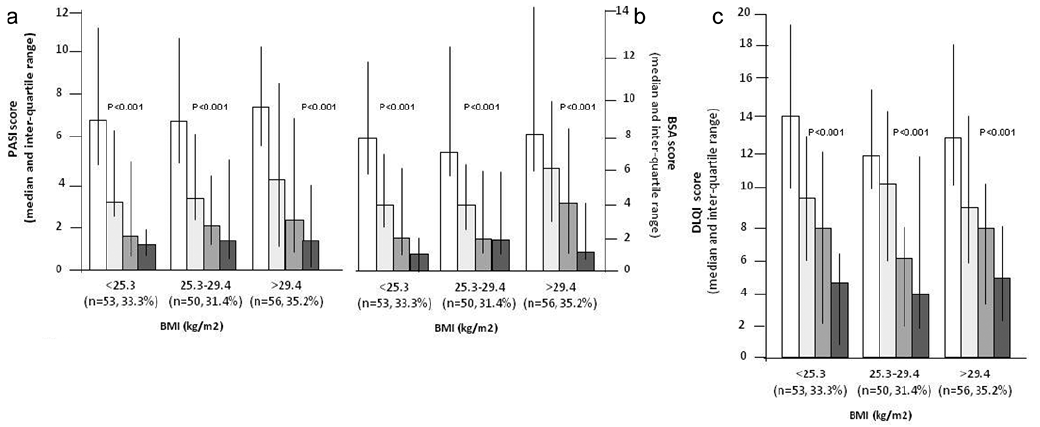 Click to show fullsize
Click to show fullsize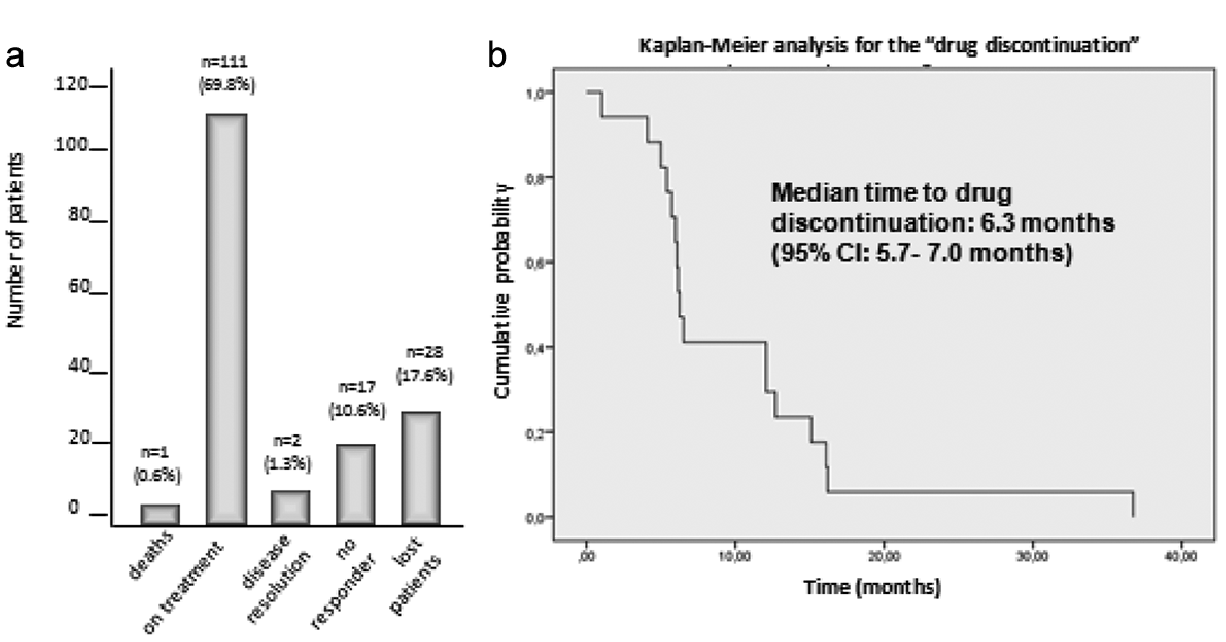 Click to show fullsize
Click to show fullsize